| MSKSONO.COM |
 |
 |
 |
 |
 |
 |
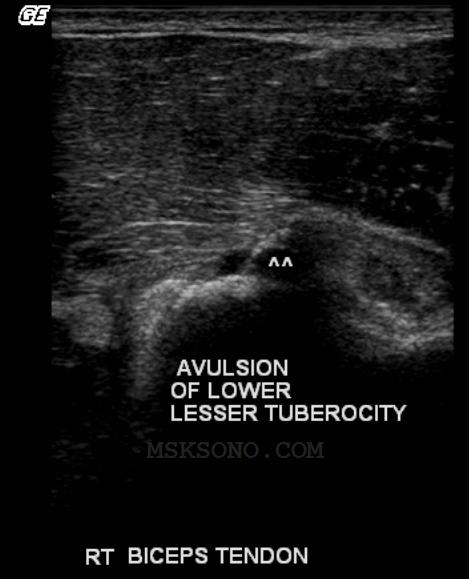
Case study involving a 16yr old football player who injured his shoulder
reaching for a fumble 3 days prior to this study. His arm was abducted above
his head, and then pulled behind him.
The father in this case refused an MRI as a prior shoulder injury had an MRI
and resulted in a negative study. Thought his son was fine when the
Radiograph showed no fracture and the patient could still raise his arm above
his head.
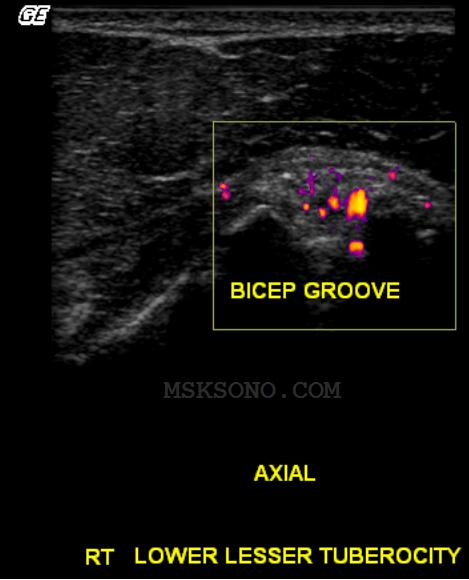
The Doctor then ordered the ultrasound appealing to the lower cost, readily
available due to the fact we are located next door to his office. The father of
the football player agreed to this, and we were all glad he did.
reaching for a fumble 3 days prior to this study. His arm was abducted above
his head, and then pulled behind him.
The father in this case refused an MRI as a prior shoulder injury had an MRI
and resulted in a negative study. Thought his son was fine when the
Radiograph showed no fracture and the patient could still raise his arm above
his head.
The Doctor then ordered the ultrasound appealing to the lower cost, readily
available due to the fact we are located next door to his office. The father of
the football player agreed to this, and we were all glad he did.
Click on any image below for larger size
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

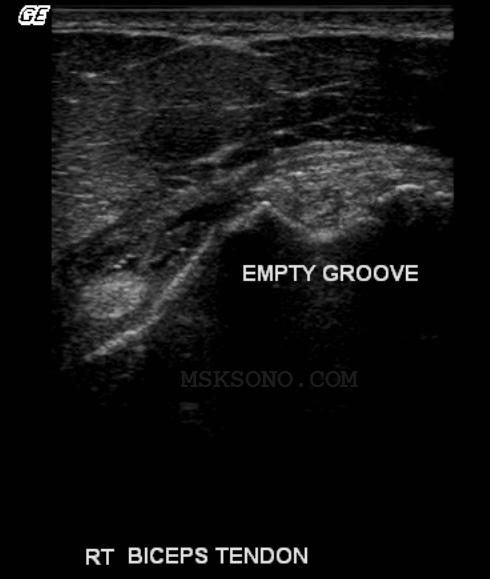


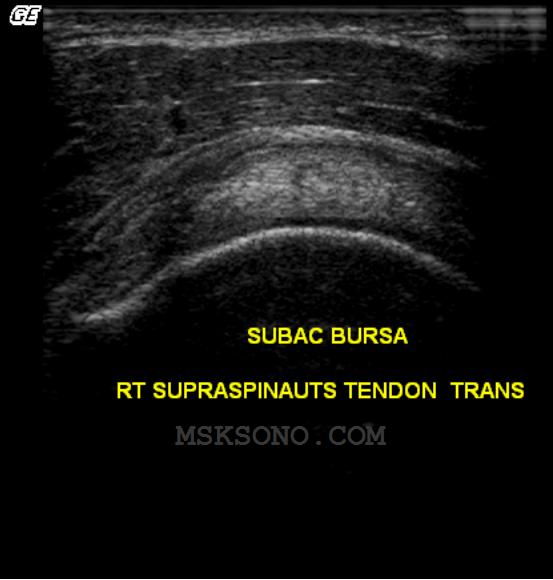



CASE STUDY: SHOULDER INJURY

10-30-2009

